Robert
@robertfm-college-com
Forum Role: Keymaster
Registered: 4 years, 3 months ago
-
Robert
KeymasterFebruary 18, 2022 at 1:58 pm #58815This is based on the Final Rule adopted by CMS adopting provisions of the 2012 NFPA Life Safety Code.
(Commentary on the web from several sources)
”
The Centers for Medicare and Medicaid Services (CMS) recently published a final rule updating fire safety requirements for healthcare facilities in an effort to increase patient safety and adapt to the needs of an aging population. The new rule adopts provisions of the National Fire Protection Association’s (NFPA) 2012 edition of the Life Safety Code (LSC), as well as provisions of the NFPA’s 2012 edition of the Health Care Facilities Code (HCFC). The 2012 edition of the LSC is more aligned with current state building codes and accreditation standards for Medicare- and Medicaid-participating facilities while the HCFC contains detailed provisions specific to healthcare and ambulatory care facilities.
Facilities affected by this rule include critical access hospitals; long-term care (LTC) facilities; inpatient hospice facilities; programs for all-inclusive care for the elderly; religious non-medical healthcare institutions; ambulatory surgical centers (ASCs); and intermediate care facilities for individuals with intellectual disabilities (ICF-IIDs). The rule includes changes to construction, protection and operational issues affecting safety from fire, smoke and panic that include the following:
- Healthcare facilities located in buildings taller than 75 feet are required to install automatic sprinkler systems by July 5, 2028.
- Healthcare facilities must also have a fire watch or building evacuation if their sprinkler system is out of service for more than 10 hours.
- LTC facilities will be able to place fixed-seating in their corridors and place certain decorations in patient rooms, such as hanging pictures. Fireplaces in smoke compartments will be permitted without a one-hour fire wall rating.
- Inpatient facility kitchen and/or cooking areas now may have an entrance from the hallway so that residents are able to make themselves a meal or snack.
- All ASCs’ doors to hazardous areas must be self-closing or must close automatically and alcohol-based hand rub dispensers may be placed in corridors to allow for easier access.
- Roller latches will be prohibited in existing and new healthcare occupancies (defined as a facility having four or more patients on an inpatient basis) for corridor doors and doors to rooms containing flammable or combustible materials. Such doors will be required to have positive latching devices instead.
- ICF-IIDs must have expanded sprinkler requirements to include habitable areas, closets, roofed porches, balconies and decks in new facilities. Heat-detection systems must be installed in attics that are not used for living purposes and sprinklers installed in attics that are used for living purposes, including storage and fuel-fired equipment.
CMS may choose not to enforce provisions of the final rule if state fire and safety codes provide equal protection or are deemed stricter, or the agency may grant waivers if the application of a provision would impose an unreasonable hardship on the facility. The effective date of the final rule is July 5, 2016, unless a specific provision states otherwise.”
-
KeymasterFebruary 15, 2022 at 2:12 pm #58638
We had discussed this in class, so I will not repeat that discussion here.
However I did find an excellent set of articles that cover many aspects of Integrated Project Delivery at the Lean Construction Institute website.
Here is a link to their “Lean Articles” page. The second tab, “Integrated Project Delivery & Strategy” has some very good articles and discussion:
-
KeymasterJanuary 23, 2022 at 4:37 pm #56850
Henry,
I’ve been doing some more research on this topic.
The electronic version I purchased access to from ASHE (Certified Healthcare Facilities Manager (CHFM) Exam Preparation Flash Cards – electronic version $40-$45) shows a 2020 copyright date. However, that being said, I do not find any material that is significantly different than what I would expect to see in earlier versions.
As to content, these flashcards seem designed to help with “recall” type questions. Thus they work as a memorization tool for learning code reference citations. Since most of the codes we are using date from 2012 (FGI 2014) there are no significant differences from earlier years.
Regarding the 2019 version that you found available. I believe you would find them useful if available to you.
A further note about purchasing this product from ASHE:
The e-version (which I purchased) provides access to view the 240 flashcards (60 for each of the 5 disciplines) for six months. It also allows you to take a “practice exam” of 100 questions one time. For $40 member $45 non-member I consider it a good value. However, I don’t consider it anywhere near a complete training program for the exam.
(Also, note that the “hard-copy” (paper) version is currently on back-order in the ASHE store and unavailable.)
-
KeymasterJanuary 20, 2022 at 10:03 am #56651
Thanks for your question!
I believe the 2019 version is the latest that AHA/ASHE has made available. (2020 and 2021 have been so upended by Covid, that there have not been code updates, etc. that would require changes to the exam. I expect that will change in 2022.)
That being said, I am not terribly impressed with them. I had recently purchased access to them. I had purchased the “electronic version” thinking it would be something like a “password protected” PDF file that I could download and use to study with. To my surprise it was only an access ID to the content on their website! On top of that it was only for a time specific period, not indefinitely.
So “buyer beware”.
That being said, students from our prior classes have shared resources that they have found that may be useful. I will attach them to this post. You are welcome to download and make use of them with the caveat that no warranty is expressed or implied.
If you have resources you would like to make available as well to other students, please feel free to upload them in a post as well.
-
KeymasterJanuary 20, 2022 at 9:50 am #56650
Thanks for your question!
As you may imagine there are really two purposes/outcomes we would expect for this course. One is the ability to pass the CHFM Exam, the second is the ability to successfully perform the job function of a Healthcare Facility Manager.
In another post, I’ve highlighted that more than half of the questions on the exam are based on the “application” of knowledge to healthcare facilities management. This type of question can not be studied for in the same manner as a “recall” question. We need to consider the broader application of our knowledge instead of a particular “point of knowledge”. Thus, it may no5t be possible to point to a specific slide and say for example “this is important for the exam”.
To the extent that we will be talking about topics related to “recall” style questions, we will make efforts to highlight that discussion as important in the context of the exam.
-
KeymasterJanuary 20, 2022 at 9:40 am #56649
Thanks for your question!
The answer is somewhat nuanced. To start with let’s look at the question type breakout that AHA provides for the exam:
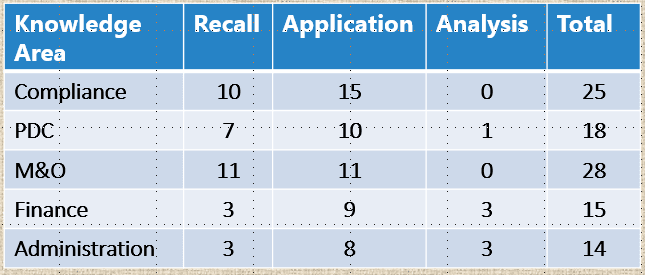
As you can see, for the compliance section they list “recall” questions and “Application” questions.
My understanding is that the “recall” questions focus on codes and standards (NFPA, ASHRAE, etc.). To a lesser extent there could be some direct mention of CMS requirements from the Center for Medicaid & Medicare Services (CMS).
However questions are also listed in this section of an “Application” nature. What this means is that you will be asked to apply this codes and standard knowledge to “real world” situations. Here, they would not be asking for chapter and verse from TJC, but would expect a good working knowledge in how that knowledge would be applied. The knowledge we discuss in the course of the Elements of Performance from TJC should provide a frame of reference for considering the complex, real world application of compliance in a healthcare setting.
I do not believe you need to be able to cite the specific TJC Standards and EPs (ie. Recall) however you do need to be able to apply codes and standards to real world problems. As such, a good working knowledge of TJC requirements is useful as a demonstrated successful approach to compliance.